Prepared by Dr. Sahin KARALAR
Epidemiology
Mechanism of Injury
Biology
History
Physical Examination
Soft-Tissue Assessment
Compartment Syndrome
Plain Radiography
Rule of Two Joints
Computed Tomography (CT)
Descriptive Classification
AO Pediatric Comprehensive Classification of Long Bone Fractures (AO PCCF)
Indications
Acceptable Alignment Criteria
Technique

Figs. 1-A through 1-D Radiographs of a 4-year-old girl who had sustained a short spiral tibial shaft fracture while skiing.
Figs. 1-A and 1-B The patient was treated with gentle closed reduction and long leg cast immobilization.
Figs. 1-C and 1-D The patient subsequently progressed to healing in anatomic alignment.
Indications
Elastic Stable Intramedullary Nailing (ESIN/TENS)
Rigid Intramedullary Nailing
Submuscular Plating
Overall Outcomes
Time to Recovery
Operative Treatment Considerations
Long-Term Follow-Up
Leg-Length Discrepancy (LLD)
Acute Compartment Syndrome
Delayed Union and Nonunion
Malunion and Angular Deformity
1.AO Foundation. (2024).Pediatric tibia, diaphysis: Diagnosis and management. AO Surgery Reference.
2.Raducha JE, Swarup I, Schachne JM, Cruz AI Jr, Fabricant PD. Tibial Shaft Fractures in Children and Adolescents. JBJS Rev. 2019 Feb;7(2):e4. doi: 10.2106/JBJS.RVW.18.00047. PMID: 30817691.
3.Waters PM, Skaggs DL, Flynn JM. Rockwood and Wilkins’ Fractures in Children. 9th ed. Philadelphia: Wolters Kluwer; 2019.
4.Bauer JM, Lovejoy SA. Toddler’s Fractures: Time to Weight-bear With Regard to Immobilization Type and Radiographic Monitoring. J Pediatr Orthop. 2019 Jul;39(6):314-317. doi: 10.1097/BPO.0000000000000948. PMID: 31169752.
5.Maleki A, Qoreishy M, Kazemi S M, Yahya G. Pediatric Tibial Shaft Fractures Remodeling After Casting. JROS 2022; 9 (2) :93-98 URL: http://jros.iums.ac.ir/article-1-2204-en.html
6.Stenroos A, Puhakka J, Nietosvaara Y, Kosola J. Treatment of Closed Tibia Shaft Fractures in Children: A Systematic Review and Meta-Analysis. Eur J Pediatr Surg. 2020 Dec;30(6):483-489. doi: 10.1055/s-0039-1693991. Epub 2019 Aug 22. PMID: 31437858.
7.Cruz AI Jr, Raducha JE, Swarup I, Schachne JM, Fabricant PD. Evidence-based update on the surgical treatment of pediatric tibial shaft fractures. Curr Opin Pediatr. 2019 Feb;31(1):92-102. doi: 10.1097/MOP.0000000000000704. PMID: 30461511.
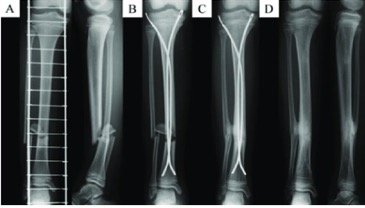
A 10-year-old girl with closed tibial shaft fracture (AO classification: 42D/4.2). (A) Preoperative anteroposterior and lateral radiographs. (B) Immediately postoperative anteroposterior radiographs. (C) 6 months after surgery, tibiofibular synostosis was detected with union. (D) Anteroposterior radiographs 14 months after surgery.
8.Miyamoto, S.; Otsuka, M.; Hasue, F.; Fujiyoshi, T.; Kamiya, K.; Kiuchi, H.; Odagiri, T.; Tanaka, T.; Nakamura, J.; Orita, S.; Ohtori, S. Associated Injury Complicated by Pediatric Lower Limb Shaft Fractures and Clinical Efficacy of Flexible Stainless-Steel Intramedullary Nailing in Children Less than 15 Years Old. Orthopedic Reviews 2021, 13. https://doi.org/10.4081/or.2021.8008.
9.Raducha, J.; Swarup, I.; Schachne, J.; Cruz, A.; Fabricant, P. Tibial Shaft Fractures in Children and Adolescents. JBJS Reviews 2019, 7, 1. https://doi.org/10.2106/JBJS.RVW.18.00047.