Prepared by Oguzhan BULUT
SUMMARY
Femoral shaft fractures are among the most prevalent pediatric orthopedic injuries and stand as the primary cause of hospital admission for orthopedic trauma in children.
While treatment remains a subject of debate, there is a modern transition from traditional non-operative methods toward surgical stabilization due to advancements in fixation techniques and bone biology.
Traditional reliance on non-operative care stems from the fact that children possess high osteogenic potential, leading to rapid fracture healing and generally favorable outcomes.
Management is highly tailored to the patient’s age and fracture morphology, ranging from a Pavlik harness or spica cast to operative fixation.
ETIOLOGY and EPIDEMIOLOGY
Mechanism of injury;
ANATOMY
Muscles
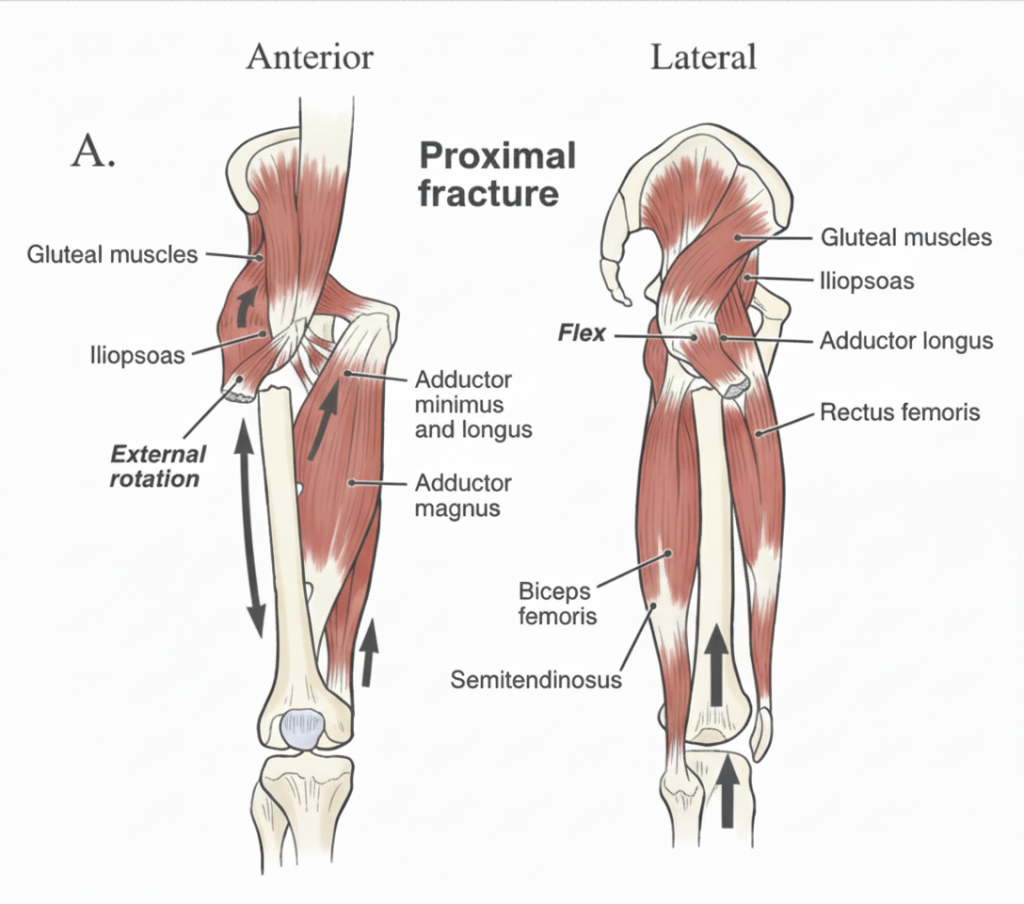
Proximal Fragment: The iliopsoas muscle exerts a specific deforming force on the proximal bone segment, pulling it into flexion and external rotation.
Distal Fragment: The adductor muscles act primarily on the distal bone segment, creating forces that result in shortening and varus (inward) angulation of the limb
PHYSICAL EXAMINATION
RADIOLOGICAL EXAMINATION
CLASSIFICATION
TREATMENT
| Patient Age Group | Fracture Characteristics | Primary Treatment Options |
| Infants (< 6 months) | All fracture patterns | Pavlik harness or Early spica casting |
| Young Children (6 months – 5 years) | Stable: Simple patterns | Early spica casting |
| Complex: Unstable patterns, polytrauma, or open fractures | External fixation or Traction followed by delayed spica casting | |
| School Age (5 – 11 years) | Length Stable: Weight < 49kg (100 lbs) | Flexible titanium nails (TENS) |
| Length Unstable: Comminuted/spiral patterns, proximal/distal locations, or regardless of weight | ORIF with submuscular bridge plating, Stainless steel Enders nails, or External fixation | |
| Adolescents (> 11 years) | Standard: Weight > 49kg (100 lbs) | Antegrade rigid intramedullary nail fixation |
| Complex: Highly comminuted, or proximal/distal metaphyseal involvement | ORIF with submuscular bridge plating |
TECHNIQUES:
This method is typically reserved for very young infants (usually under 6 months old).
Spica casting is a common definitive treatment for toddlers and young children.
In modern practice, external fixators are primarily indicated for complex scenarios where internal fixation or casting is not ideal. These include:
When you mention the “natural bend of the femur,” surgeons often refer to this as the anterior bowing of the femoral shaft. If you are using a straight LC-DCP, ensuring that longitudinal contouring matches this bow is critical to avoid “propped” reductions or malalignment.
Could you rearrange these sentences and give them back to me?
5.Flexible Intramedullary Nail (Titanium Elastic Nail)
6.Antegrade Rigid Intramedullary Nail Fixation
Surgical Approach & Entry Points
Instrumentation & Insertion
Complications
Osteonecrosis (AVN) Risks
Proximal Femur Deformities
Greater trochanteric insertions can lead to secondary deformities, including:
Outcomes
COMPLICATIONS
1. Limb-Length Inequality (LLI)
2. Osteonecrosis & Vascular Risks
3. Nonunion & Malunion
References
Flynn JM, Skaggs DL, Sponseller PD, et al. The treatment of pediatric femoral shaft fractures. J Am Acad Orthop Surg. 2015;23(11):e1–e11.
Beaty JH, Kasser JR. Rockwood and Wilkins’ Fractures in Children. 8th ed. Wolters Kluwer; 2015.
Kocher MS, Sink EL, Blasier RD, et al. Treatment of pediatric diaphyseal femur fractures. J Am Acad Orthop Surg. 2009;17(11):718–725.
American Academy of Orthopaedic Surgeons. Clinical Practice Guideline: Pediatric Diaphyseal Femur Fractures. AAOS; 2020.
Flynn JM, Hresko T, Reynolds RA, et al. Titanium elastic nails for pediatric femur fractures. J Pediatr Orthop. 2001;21(1):4–8.
Ligier JN, Metaizeau JP, Prévot J, Lascombes P. Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br. 1988;70-B:74–77.
Luhmann SJ, Schoenecker PL. Complications of titanium elastic nails for pediatric femoral shaft fractures. J Pediatr Orthop. 2003;23(4):443–447.
Kocher MS, Kasser JR. Orthopaedic aspects of child abuse. J Am Acad Orthop Surg. 2000;8(1):10–20.