Prepared by Dr. Ahmet Mucteba YILDIRIM
Overview
Clinical Presentation
Physical Examination
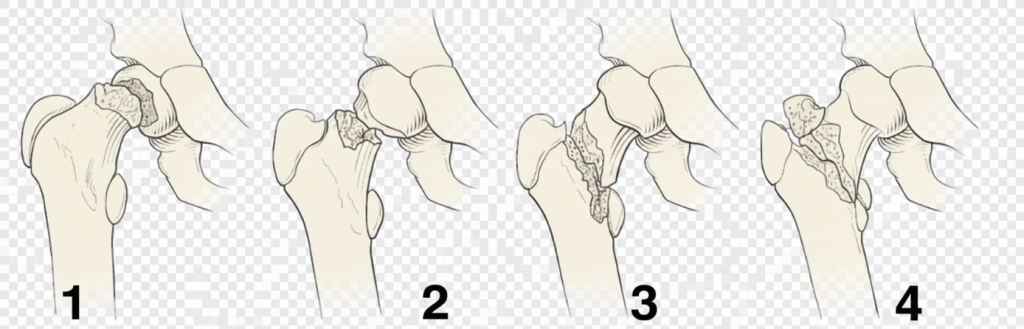
Delbet Classification and Treatment Approaches
The incidence of AVN decreases as the fracture line moves distally.
Type 1: Transphyseal Fractures (Highest AVN Risk)
Type 1 epiphysiolysis. Unlike SCFE, it involves higher energy and no prodromal period. It may be seen in newborns with breech presentation and be misdiagnosed as congenital hip dislocation. It may be seen during reduction of hip dislocation.
Treatment: Non-repetitive closed reduction followed by percutaneous fixation is performed. If reduction cannot be achieved, open reduction (using Moore or Smith-Petersen approaches) is executed.
Implant Selection: K-wires for children under 4 years; 4.0 mm screws for ages 4–7; 5.0 mm or 6.5 mm cannulated screws for those over 7 years.
To reduce the risk of AVN, hematoma aspiration and pelvic-pedal casting (hip spica) are recommended.
Type 2: Transcervical Fractures (Most Common – 50%)
Fixation is recommended even in non-displaced cases to avoid complications. Forceful closed reduction should be avoided due to AVN risk; open reduction via anterior or anterolateral approach should be performed if necessary.
In adolescents, at least two screws should be placed to provide compression. If the Pauwels angle is high or the fracture is close to the head, crossing the physis should not be avoided to ensure union. 6–12 weeks of pelvic-pedal casting follows treatment.
Type 3: Cervicotrochanteric Fractures
While the incidence of AVN is lower than in Type 2, the risk of coxa vara is similar. Surgical treatment is indicated for all displaced fractures and for non-displaced fractures in children over 6 years old. Locking plates can be used to prevent varus collapse; otherwise, cannulated screws with a hip-spica cast are applied.
Type 4: Pertrochanteric Fractures: This group has the lowest observed risk of AVN.
Complications and Management
AVN (Avascular Necrosis): Incidence rates for Type 1, 2, 3, and 4 are 38%, 28%, 18%, and 5%, respectively. Risk increases in Type 1–2 fractures, patients over 12 years old, and cases where intervention occurs after 24 hours. Capsular decompression is recommended to reduce this risk. Type 1 (total AVN) is the most common and has the worst prognosis.
Coxa Vara: Observed in 10–32% of cases. It results from inadequate perioperative reduction, loss of postoperative reduction (in groups without hip-spica), or premature physeal arrest. Pauwels valgus osteotomy is recommended when the neck-shaft angle falls below 110 degrees.
Non-Union: Occurs in 6–12% of cases. Risk increases with inadequate reduction, distraction at the fracture line, or a Pauwels angle >50 degrees. For patients under 10, iliac autografting and compressive screw fixation are recommended; for those over 10, subtrochanteric valgus osteotomies (with DHS or locking plates) are preferred to improve weight distribution.
Premature Physeal Arrest: Since the proximal femoral epiphysis contributes only 15% to overall growth, serious limb length discrepancy (LLD) is usually not seen. Screws penetrating the physis increase this risk.
Key principle: AVN risk decreases as the fracture line becomes more distal (Type I highest → Type IV lowest).
Primary goals: early diagnosis, anatomic reduction, stable fixation, and complication prevention.